Woman 65 yo, epigatric pain for one week, cannot eat and no fever.
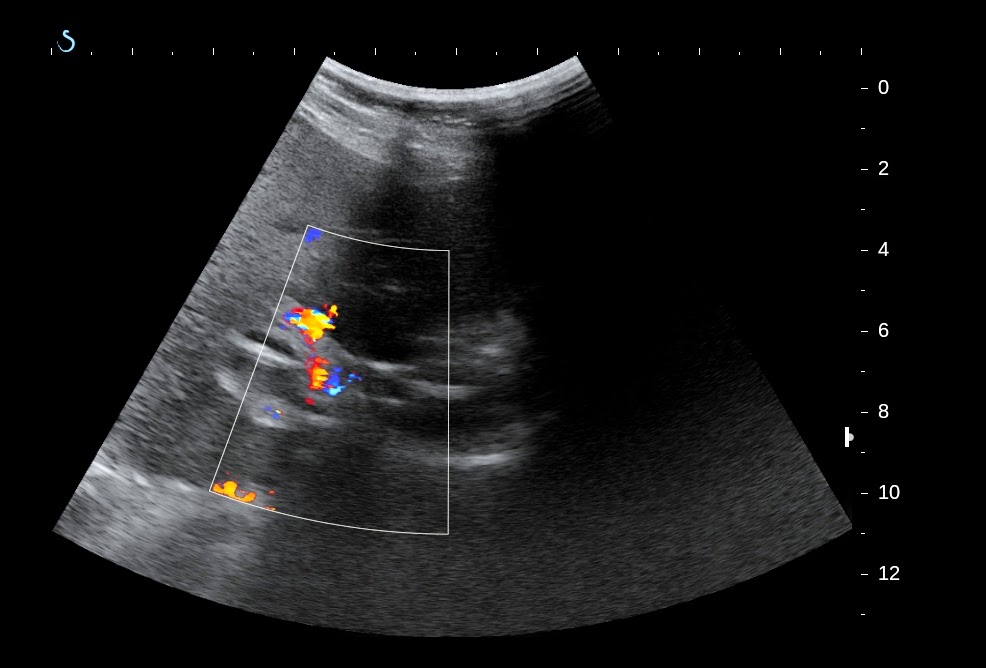
Ultrasound of abdomen in decubitus position detected vena porta thrombosis and some white lines intra portal vein which came from the wall of gastric antrum (see 4 ultrasound pictures in ventral view).
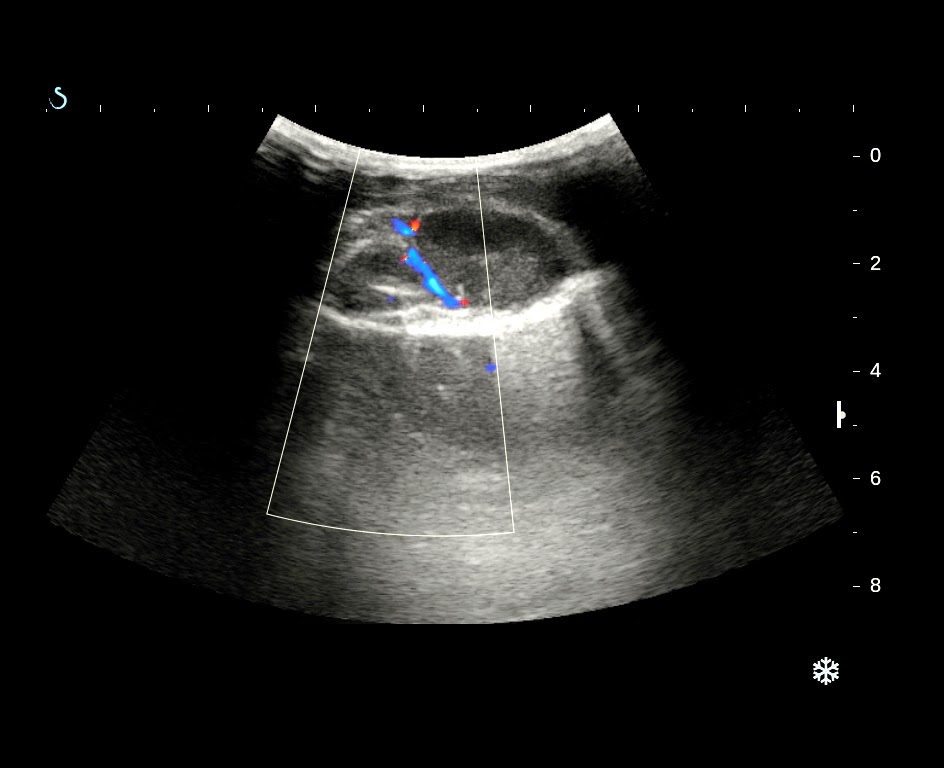
For clear viewing of portal vein we scanned the liver by sitting position and dorsal view.
Portal vein was in distension, no flow due to thrombosis, and in crossed section of portal vein we detected a white foreign body.( 2 pictures with sitting position scan ).
MSCT with CE for evaluation portal vein found out the foreign body which length of 5 cm intra left branch of portal vein and one another end was intra gastric antrum wall.
The foreign body was covered by thrombosis intra left branch of portal vein (see 3 CT images).
Blood tests confirmed infection with rising WBC and high CRP, no abnormal coagulation test.
With the past history of ultrasound scanning in ventral and dorsal views, MSCT and blood tests, the first choice of diagnosis was intraportal vein foreign body, which was liked toothpick in penetration the gastric wall and entering liver to left branch of portal vein, that caused portal vein thrombosis.
What is your suggestion and planning of treatment for the female patient?
FEEDBACK=
An anouncement about case 299 of MEDIC on Google web after the case was posted for 30 minutes.









.jpg)
.png)

.jpg)












.png)





















































































.PNG)
















































.jpg)