PLS DOWNLOAD THE LINK for PICTURES
Lady 24 yo, 5 years before fracture of left femoral head, and now fractures of 2 bones of right forearm by falling trauma [see photo].

X-rays of pelvis bone made pointed osteoporosis of bone .

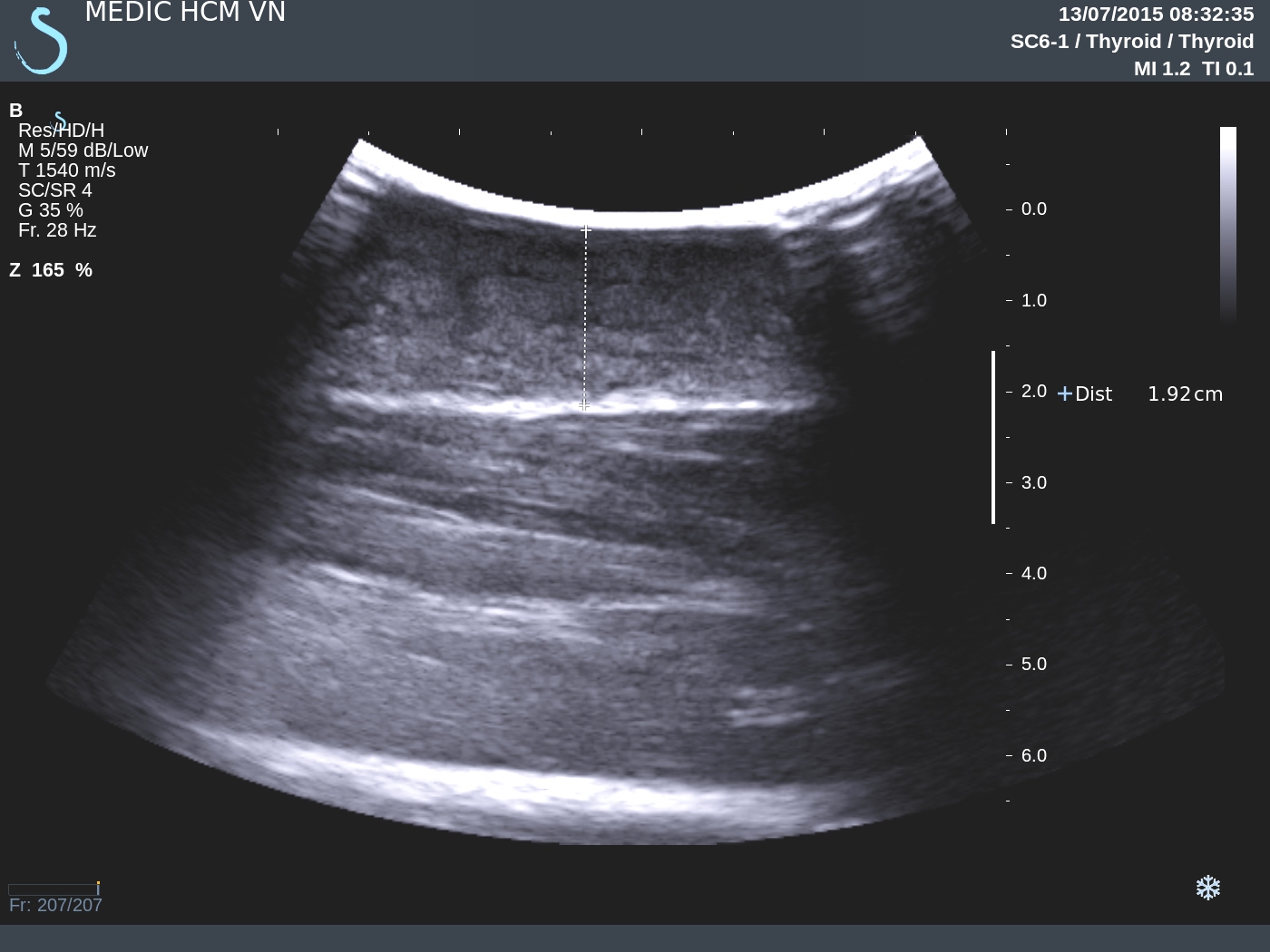
For screening, ultrasound of the neck detected one ovoid mass, size of 3-2cm, hypoechoic at the lower pole of the thyroid gland, and hypervascular on Doppler.




Sonologist suggested PTA for the case.
Osteogram BMD showed very lower bone index.

Blood tests = PTH very high and elevated calcium.

Do you make first choice of diagnosis of PTA?
OPERATION of RIGHT LOBECTOMY.THIS TUMOR WAS WELL BORDERED, SOFT TISSUE. ( see MACRO1,2).
![]()
![]()
![]()
OPERATION of RIGHT LOBECTOMY.THIS TUMOR WAS WELL BORDERED, SOFT TISSUE. ( see MACRO1,2).


MICROSCOPIC REPORT WAS PARATHYROID ADENOMA.
.jpg)
REFERENCE

























.jpg)