A 31-year-old male patient complained about 3-day mild fever, right subcostal abdominal pain. He did not have any other symtomps such as voimiting, diarrhea and no history of abdominal surgery, trauma, liver biopsy or alcohol abuse. On physical examination, no mass in the right subcostal. B-mode ultrasound (US) findings showed a cystic structure (21x21mm) in the sixth segment, it communicated with 2 parallel –dilated - tubular - structure (d = 8 and 9mm) originated from the right portal vein and right hepatic vein.
![]() Doppler US showed yin-yang sign, right portal vein flow and right portal vein flow in the cystic structure.
Doppler US showed yin-yang sign, right portal vein flow and right portal vein flow in the cystic structure.
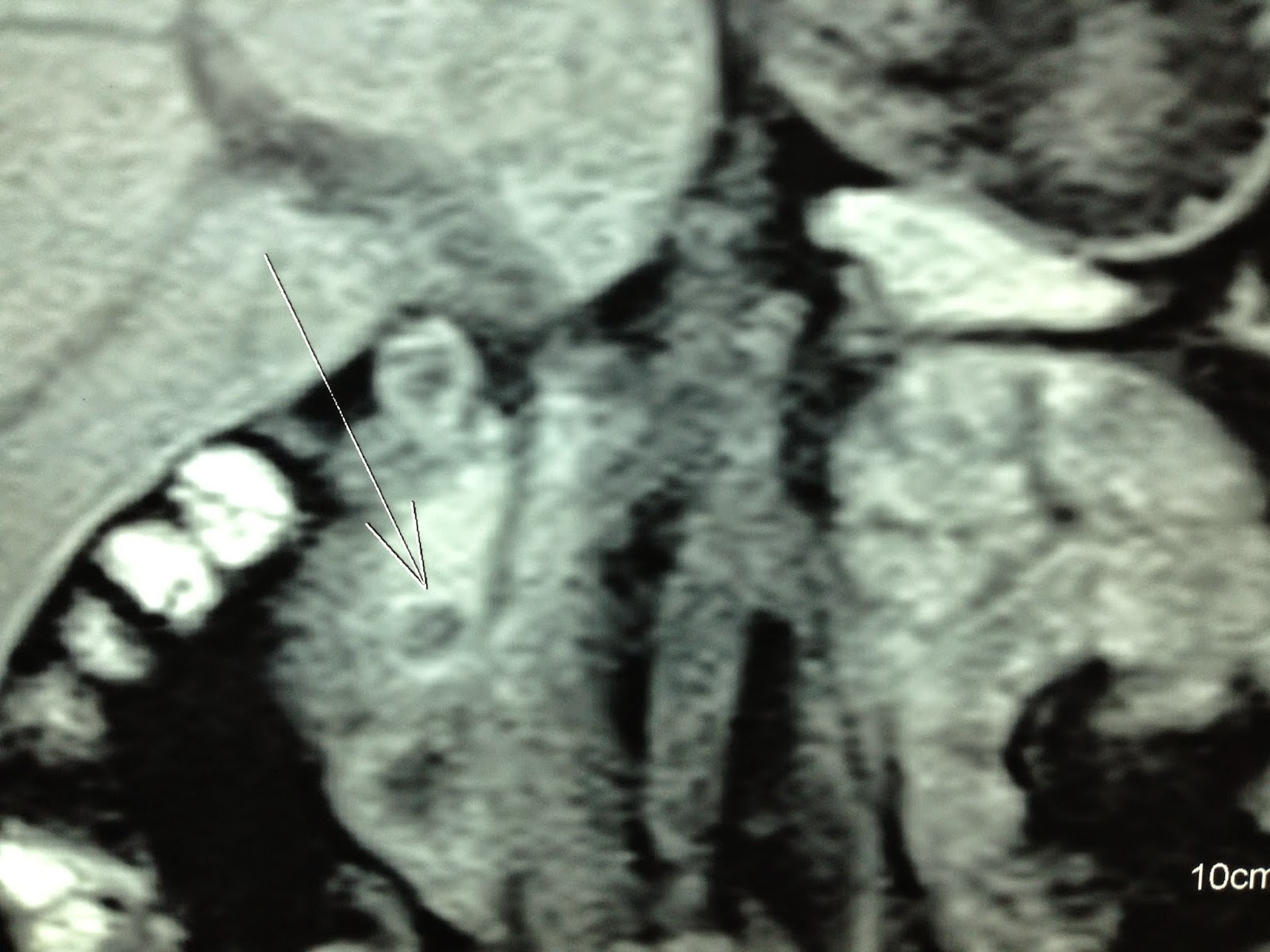
![]() MSCT Angio comfirmed the AVM in right lobe of liver.
MSCT Angio comfirmed the AVM in right lobe of liver.
![]()
![]()
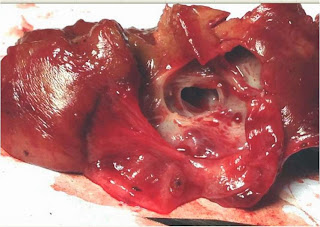
![]() The patient underwent an abdominal laparoscopic surgery for resection the AVM. In the course of operation, surgeon saw the sac pulsating.
The patient underwent an abdominal laparoscopic surgery for resection the AVM. In the course of operation, surgeon saw the sac pulsating.
![]()
![]()
![]() The patient remains well post-op.
The patient remains well post-op.
Microscopic result is concordant with hepatic AVM.
![]()







Microscopic result is concordant with hepatic AVM.











.jpg)
.jpg)































.jpg)
.jpg)


























































.jpg)
.jpg)
.jpg)
.jpg)
.jpg)


.jpg)
.jpg)


.jpg)
.jpg)



















.jpg)




