Thyroid Toxicosis Periodic Paralysis
Man 47 yo, 3 times paralysis at get up in the morning, he came to hospital for emergency perfusion potassium and to MEDIC for check- up.
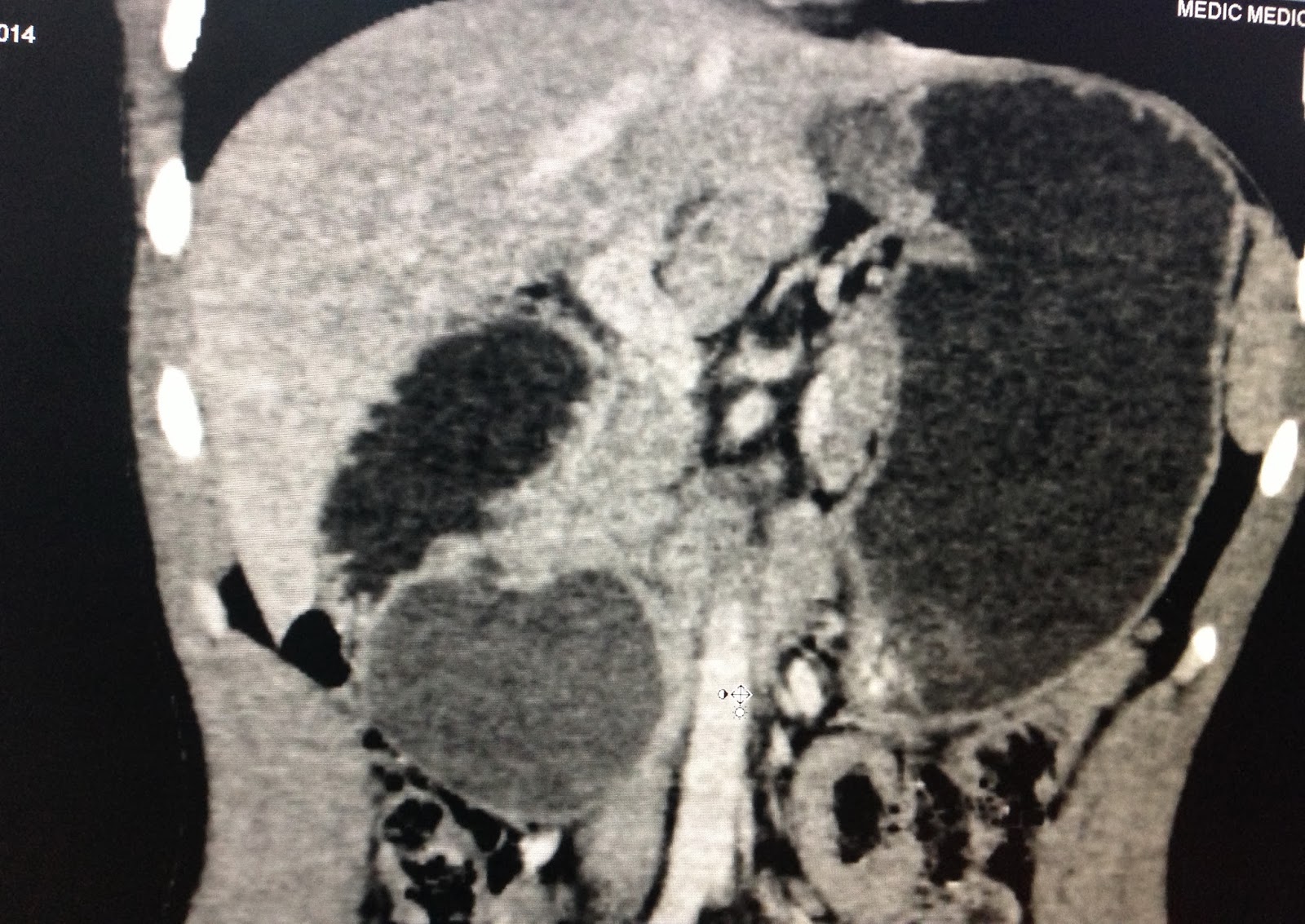
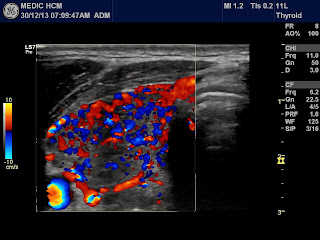
Ultrasound of abdomen no abnormal detected, no adrenal tumor, but ultrasound of thyroid gland is black , CDI hypervasular , typical of hyperthyroidis .and soft with elastoscan.



Blood test are very low TSH , high T3, T4, TPO.

Thiscase isTpP. Medical treatmentof anti thyroidism is requested.
REFERENCES:
REFERENCES: