A 29 year-old male patient complains: for six months bloating of the abdomen, non deep ache, difficulty in eating and digesting food and having a mass of 150x200mm in his epigastric region. He had a trauma of epigastric region by traffic accident seven months ago and had been operated for it.
Ultrasound examination : Cross-sectional images of the mass in epigastric region. It was a large anechoic mass with posterior acoustic enhancement, smooth contour, unilocular, no Doppler signal, size of 145x134mm, was thought to be a pseudocyst which had pressed on nearby organs (liver, stomach). It was a pancreatic pseudocyst but having a differential diagnosis of liver cyst.

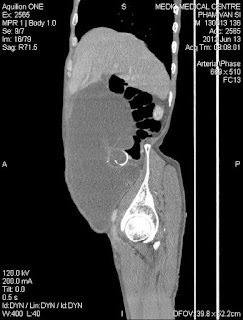
MSCT examination:
MSCT showed a well-defined unilocular pseudocyst in the pancreatic head and body, thin wall, size of 85x138mm.

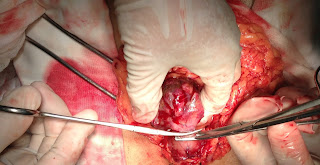
Operation:
It was pancreatic pseudocyst, wallthickness of 7mm,filled yellowish fluid. Surgical drainage of the pseudocyst, which involves making a connection between the cyst and thejejunum (Roux-en-Y anastomosis).

Microscopic report:
Pancreatic pseudocyst.

Discussion:
Pancreatic pseudocyst caused rarely by trauma and frequently happens in children. This case was a large pancreatic pseudocyst in adult due to trauma. Ultrasound was confused with a liver cyst and priority of was MSCT higher than. In this case, surgery asked for fluid analysis but forgetting of counting amylase enzyme in withdrawn fluid, but we had microscopic report of specimen to confirm a pancreatic pseudocyst.
References
Dapo Popoola, Mary Ann Lou, and Edward H. Sims. Traumatic Pancreatic Pseudocysts .J Natl Med Assoc. 1983 May; 75(5): 515–517.
Griffith, Antonio, Wong, Lee Chu, Levine, Ho, Paunipagar. Expertddx ultrasound. Amirsys. 2010. Section 5:2-3.
Hassan A El Musharaf, Mohamed A Al Auriefi. Traumatic pancreatic pseudocyst. The Saudi Lewis G, Krige JE, Bornman PC, Terblanche J. Traumatic pancreatic pseudocysts. Br J Surg. 1993 Jan; 80(1):89-93.