Neonate female 02 day-old detected one mass in perineum, size of 10cm, soft in palpation [see 2 fotos].


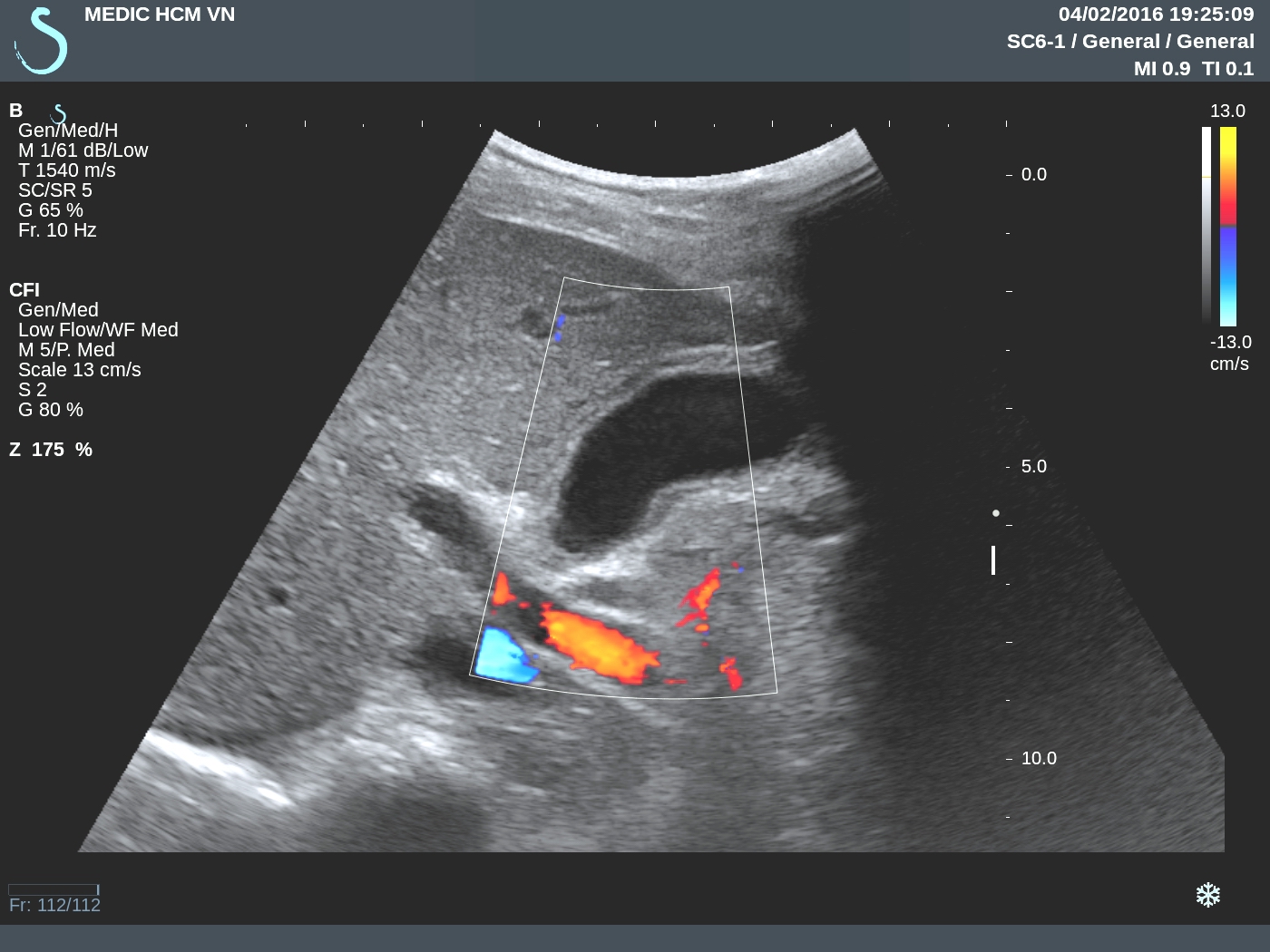
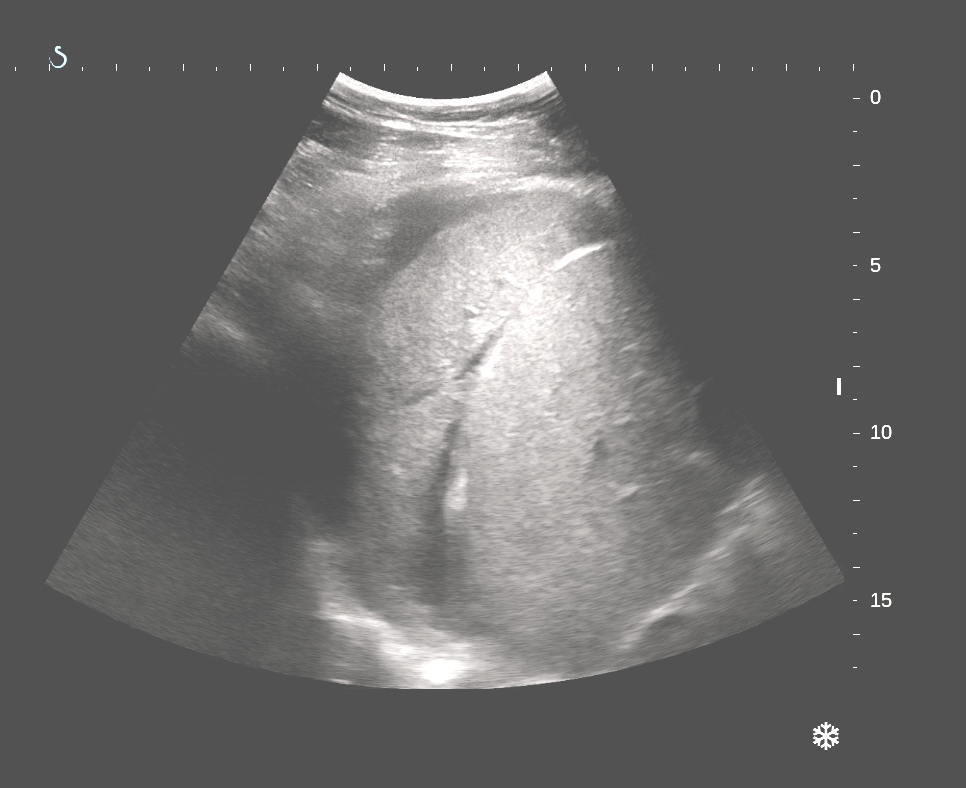
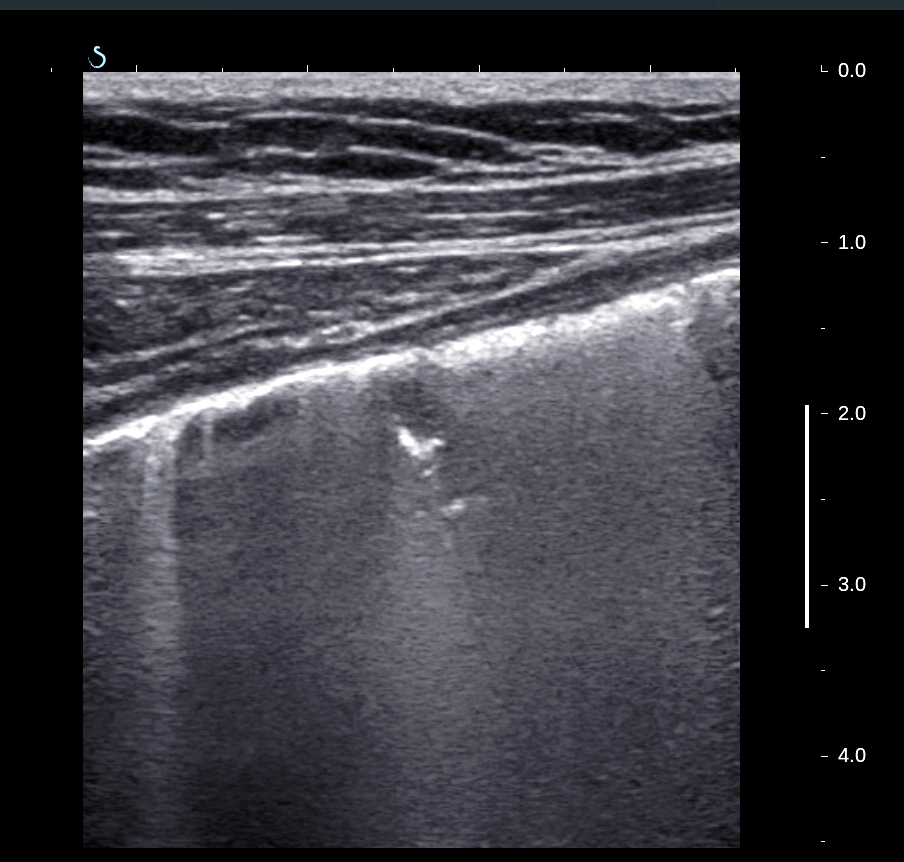
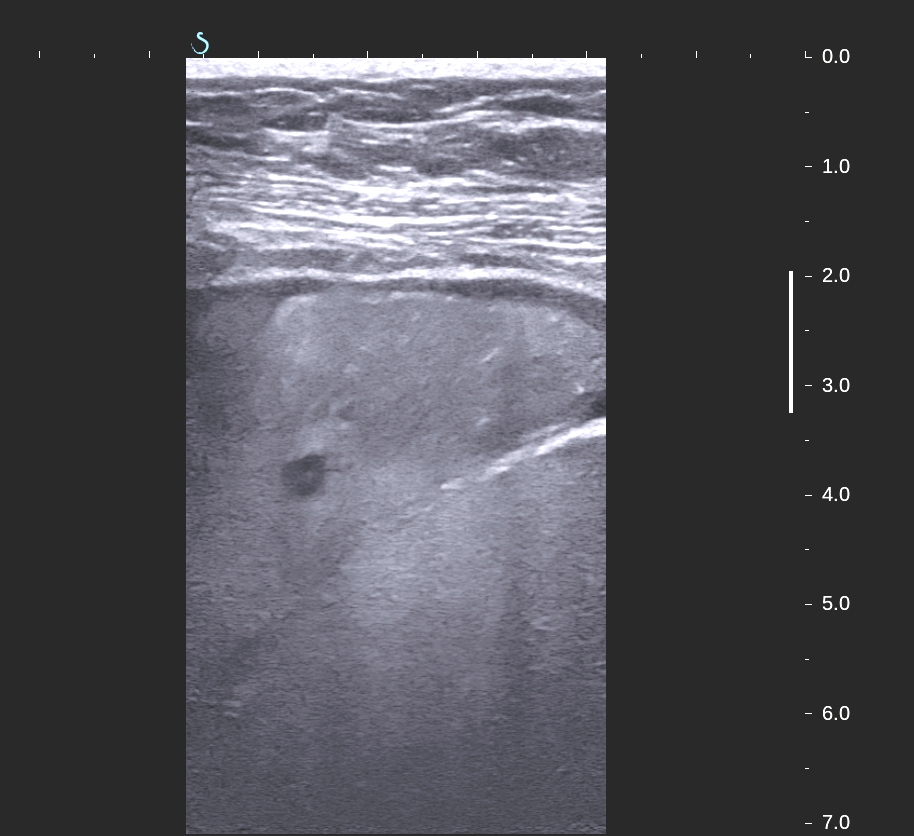
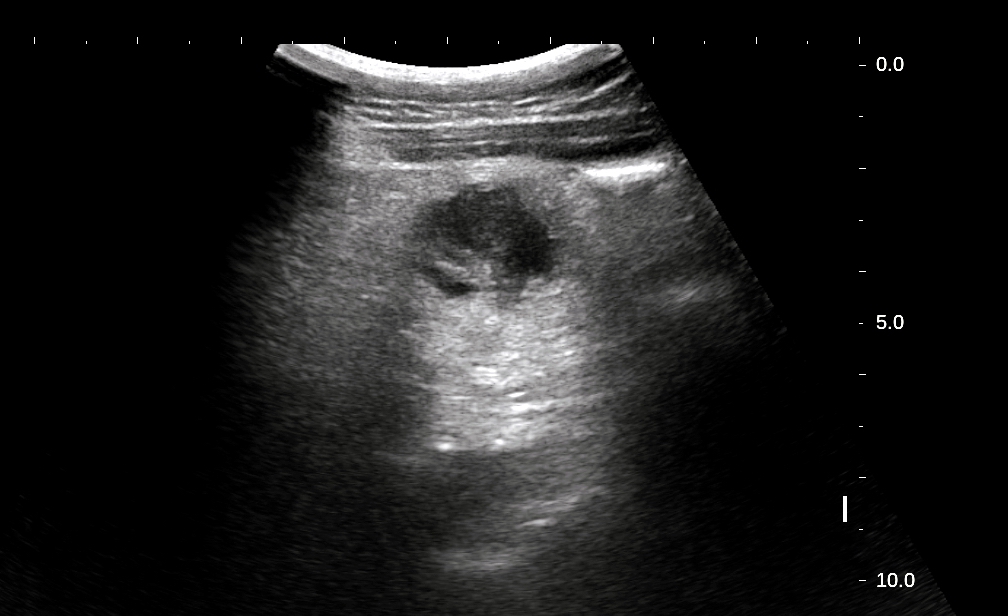
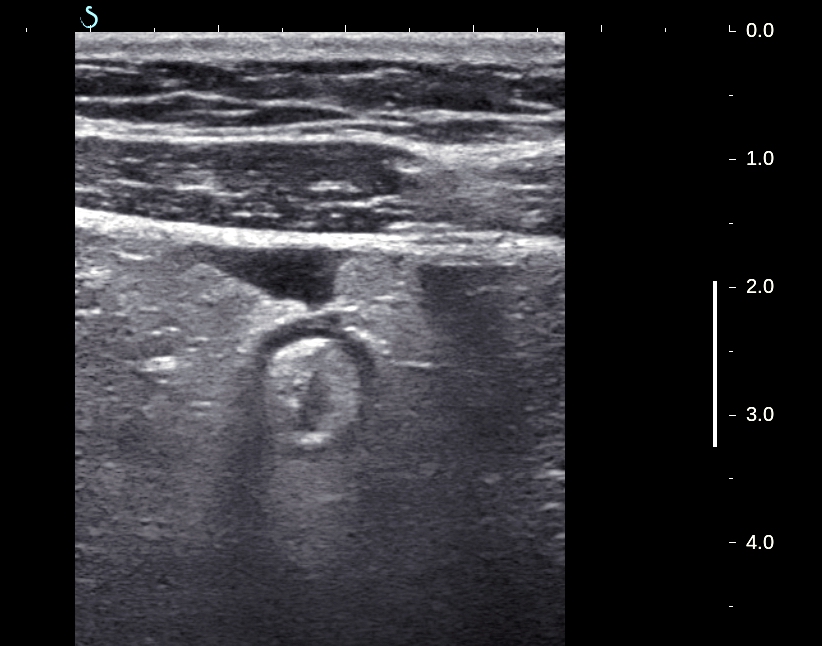
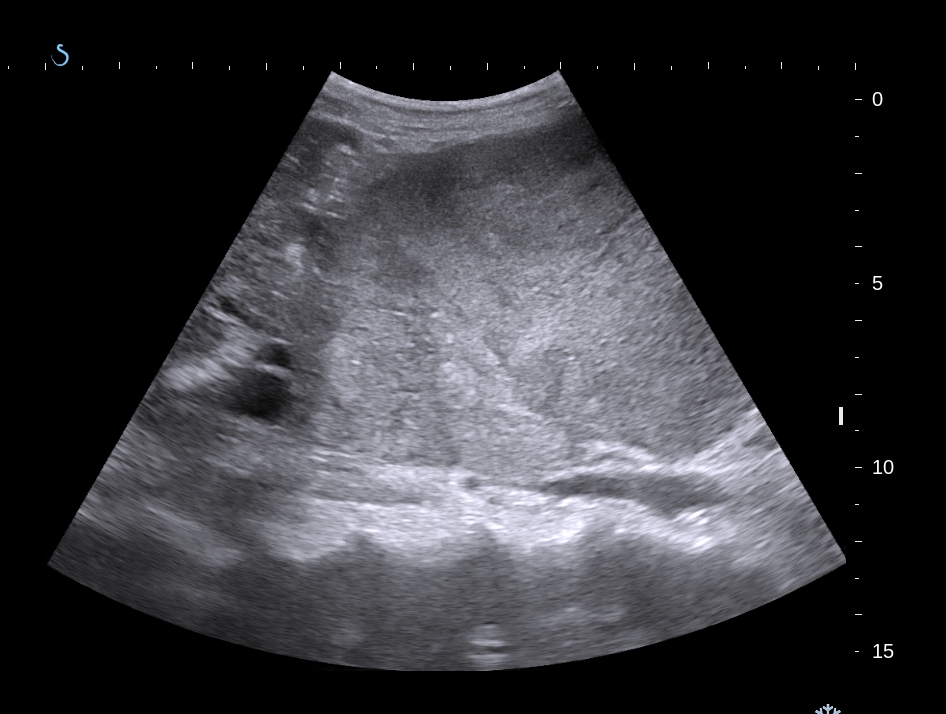
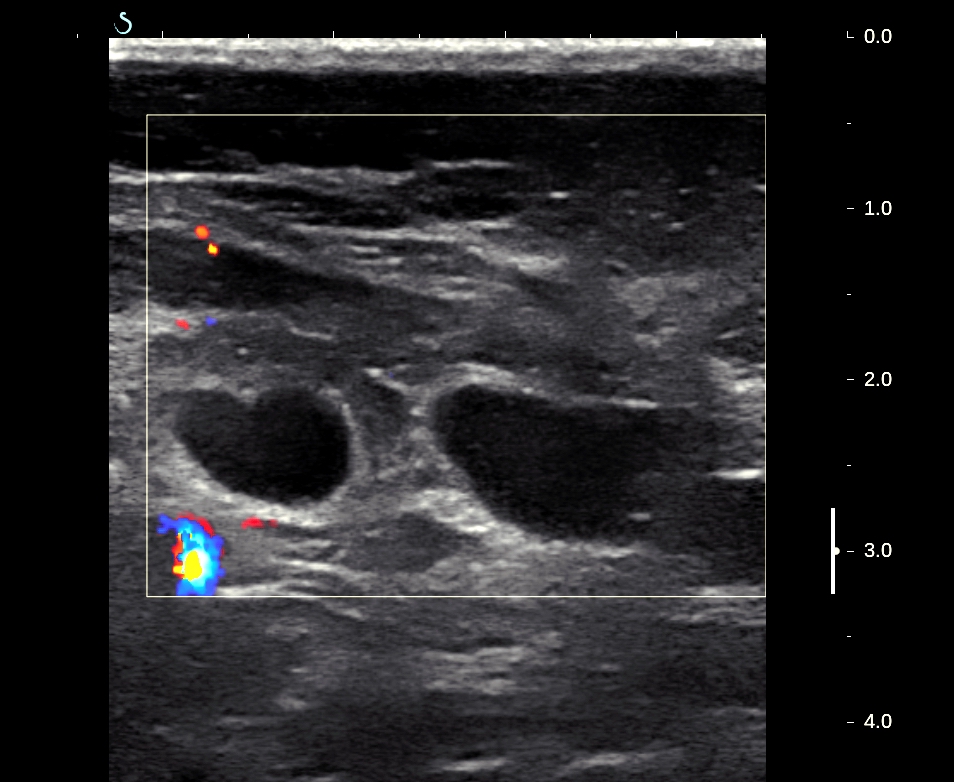
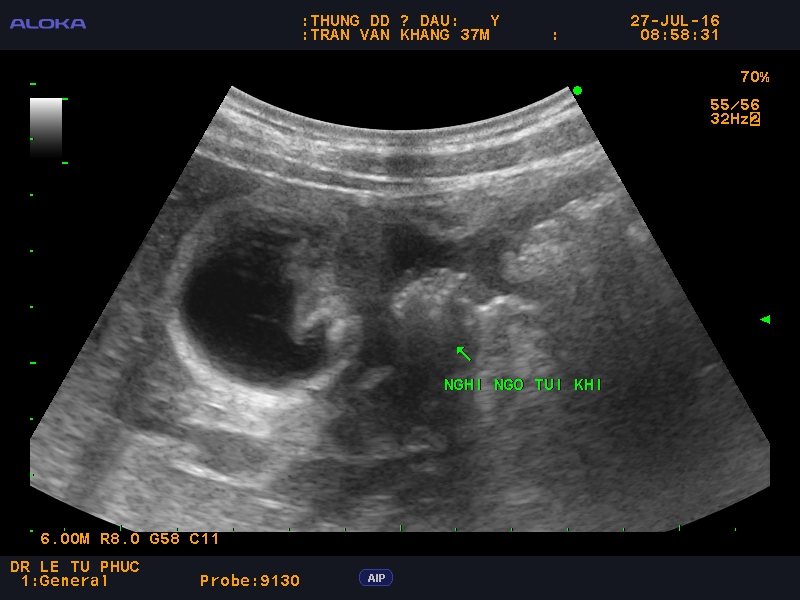
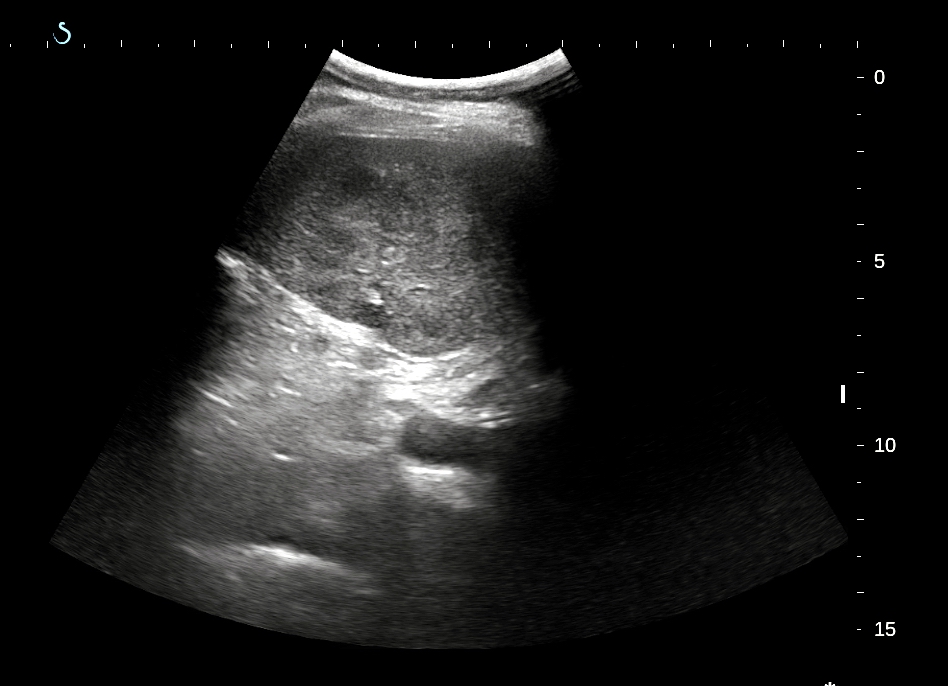
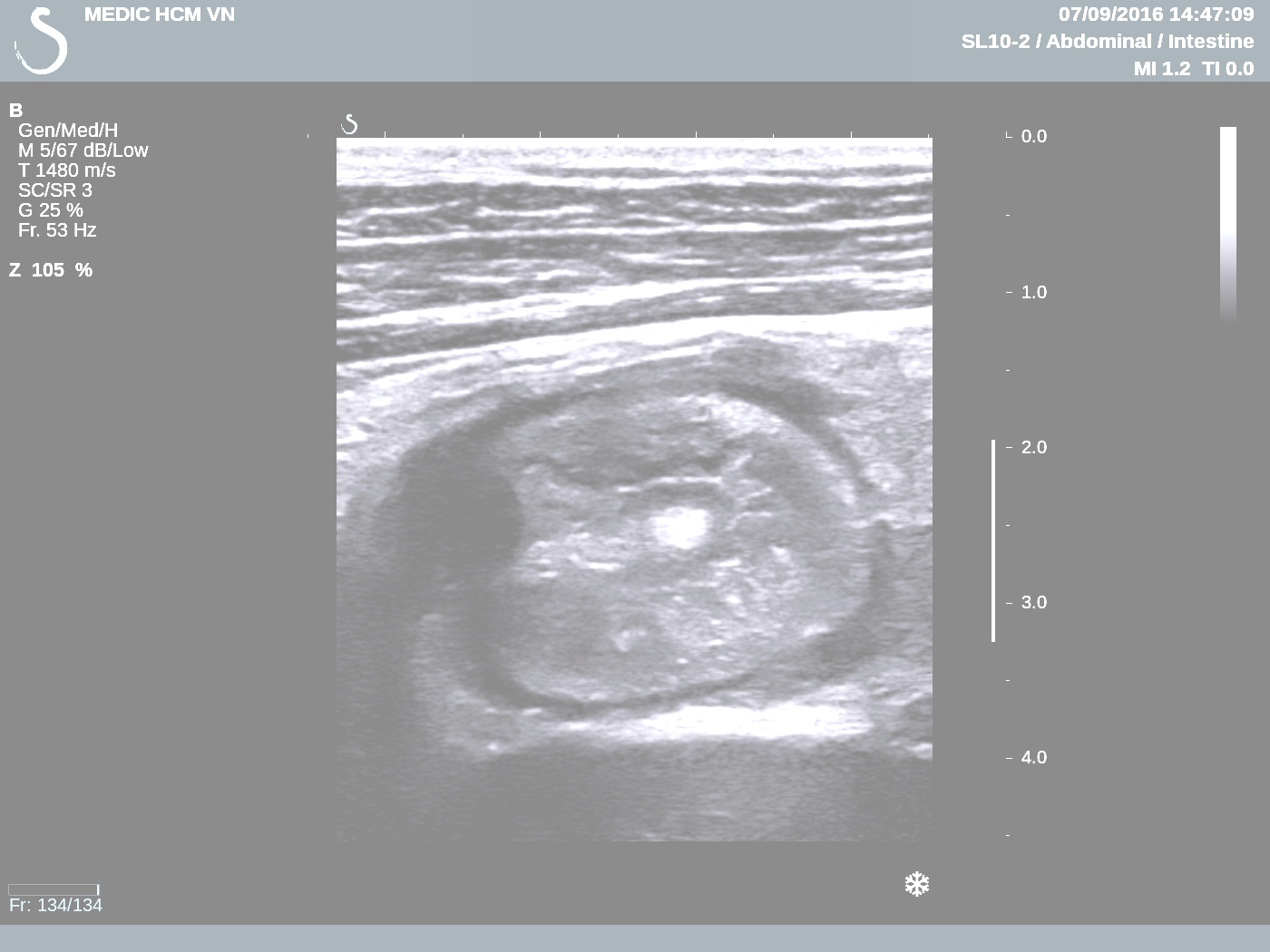
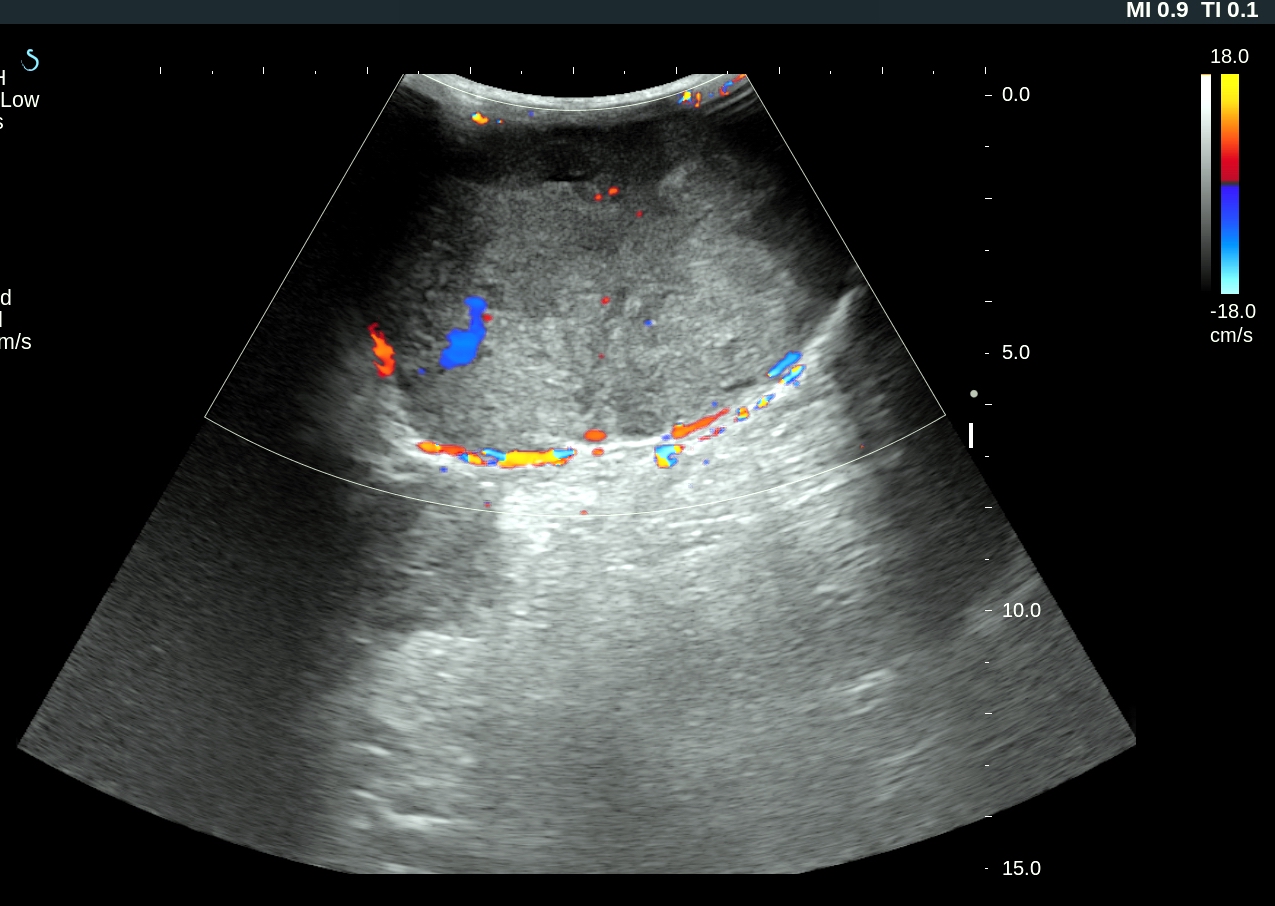
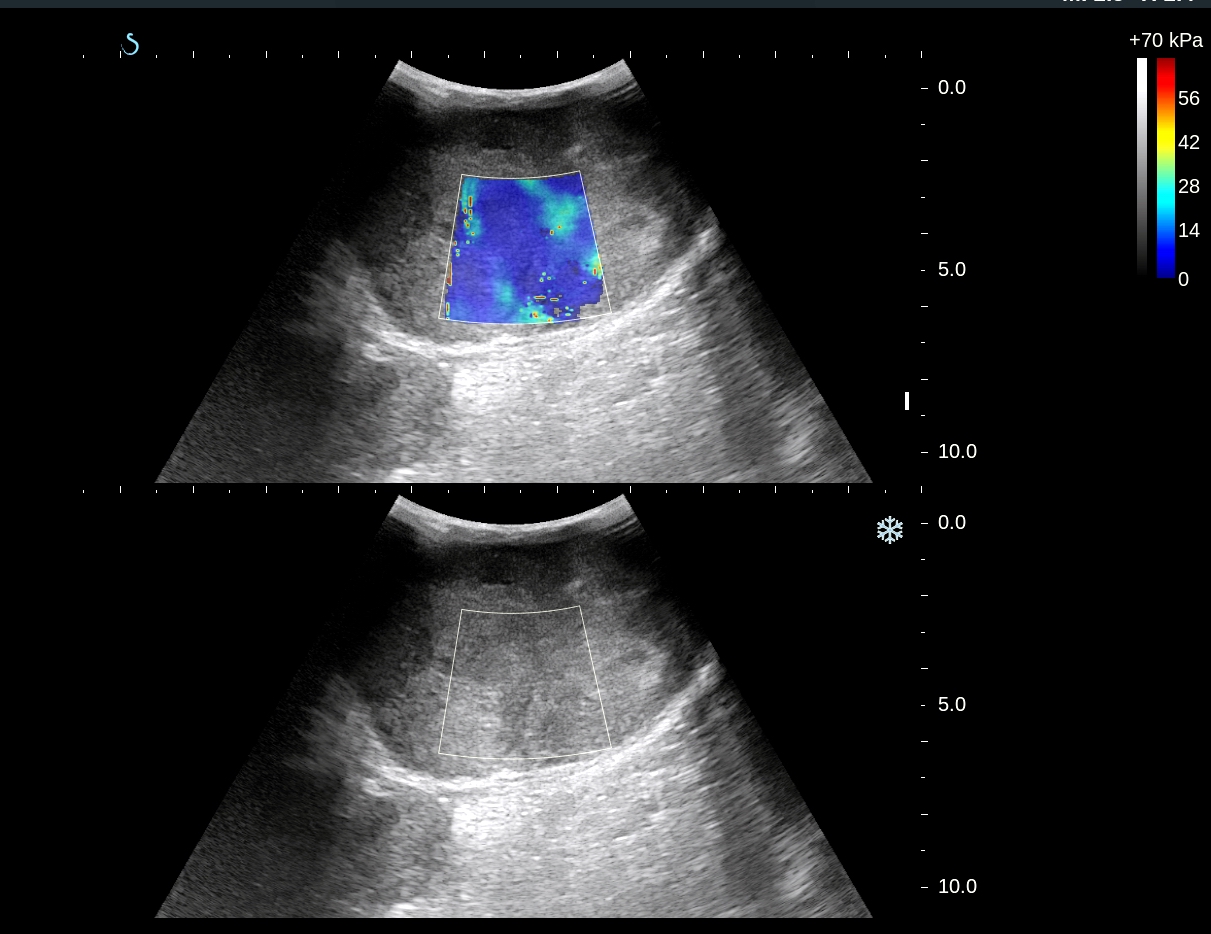
Ultrasound scanning of this mass= US1: structure of this mass is cystic septation with solid part.

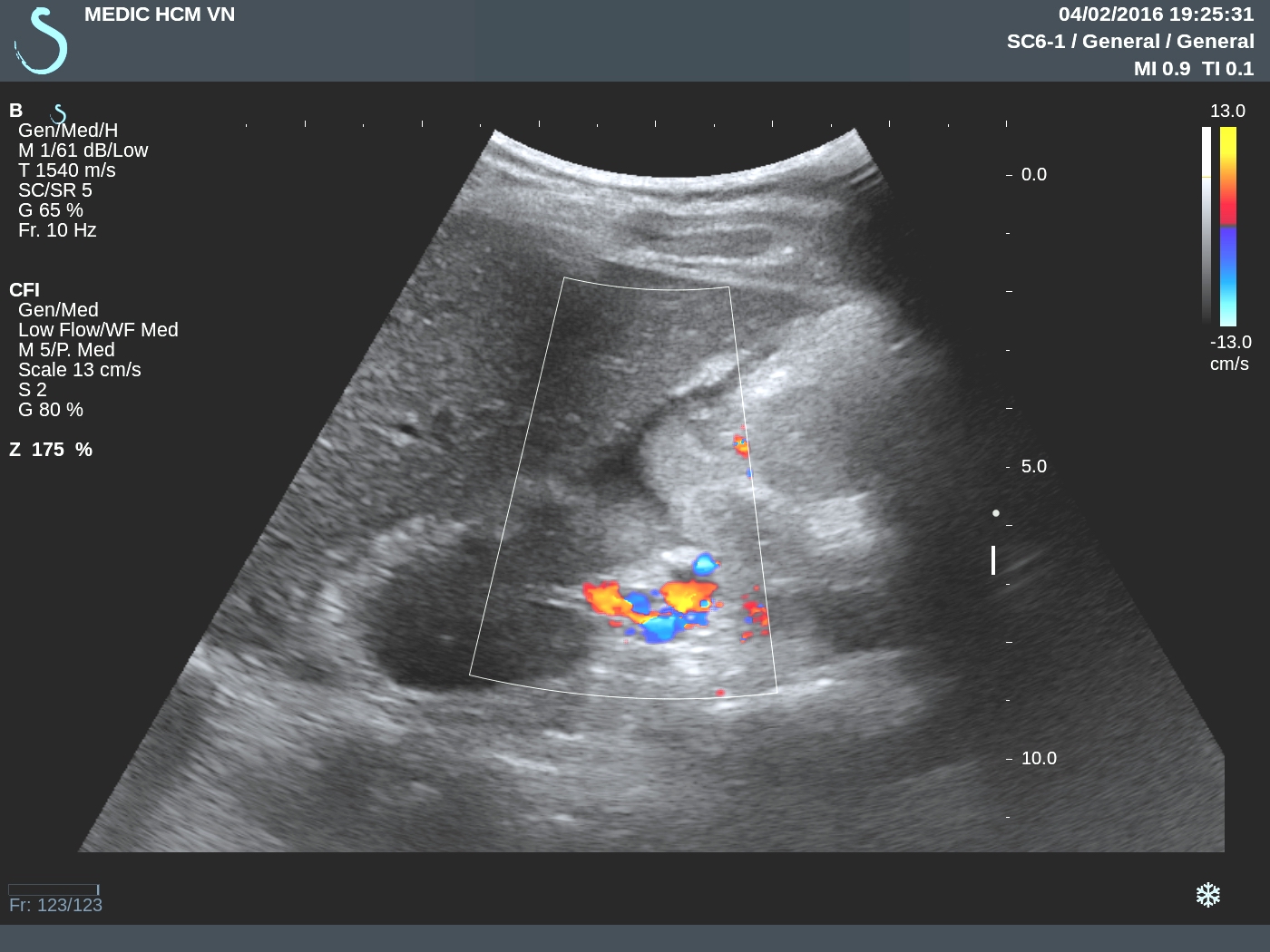
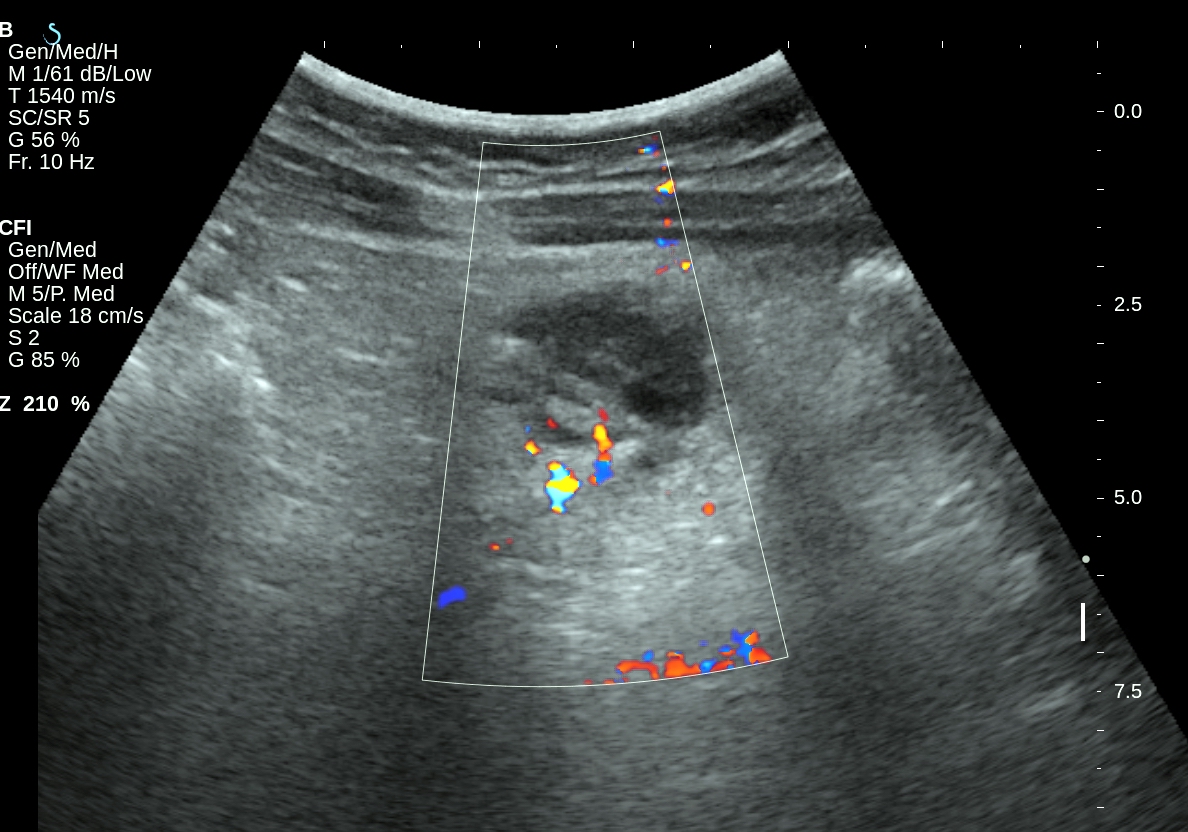
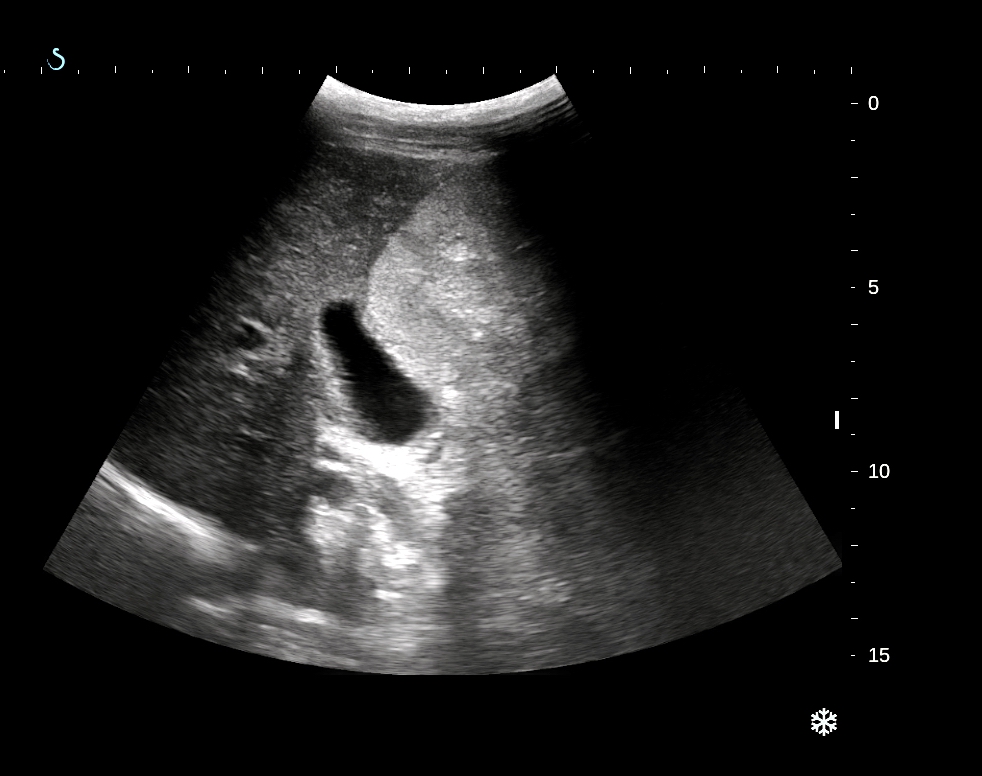
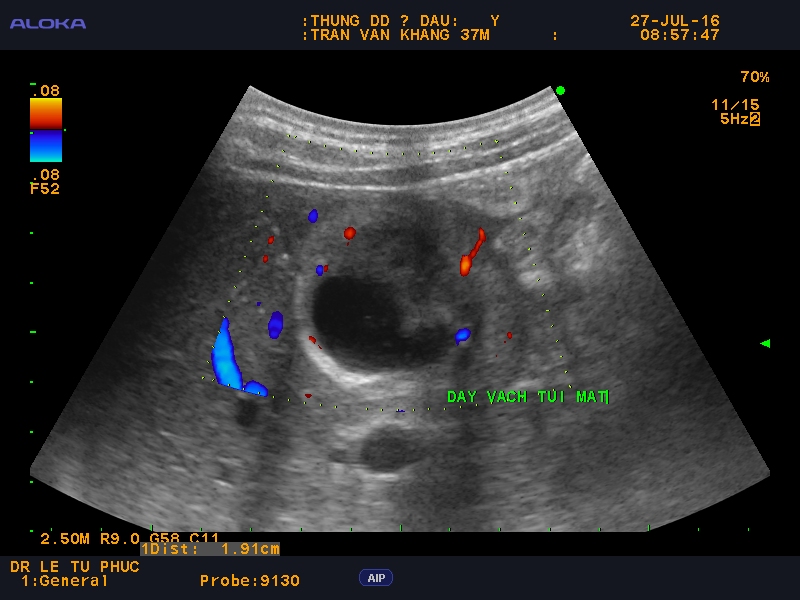
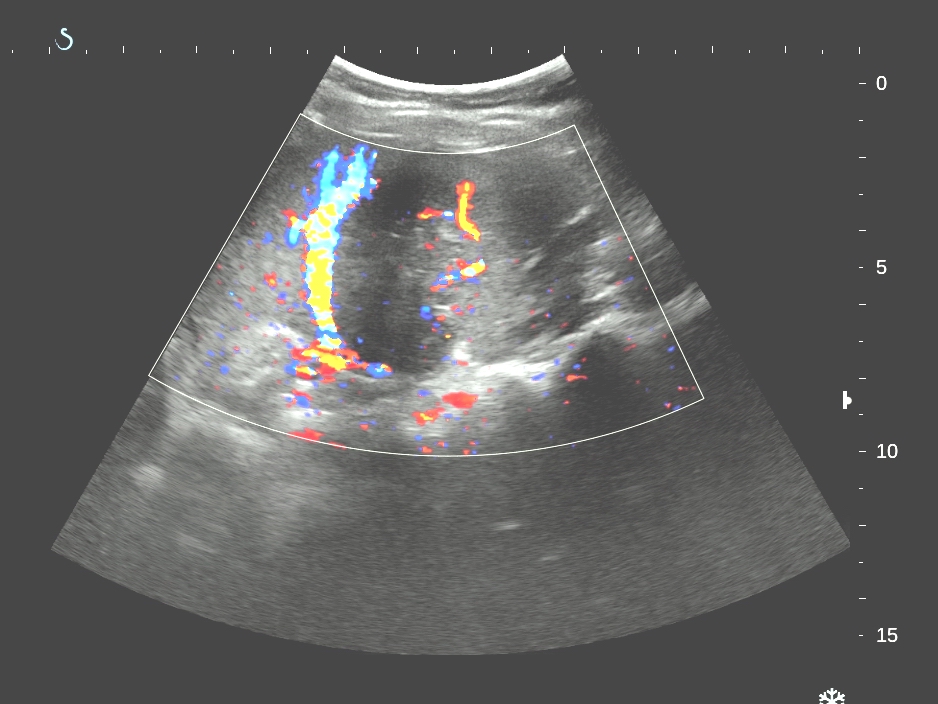
US 2 : vessels in septation.

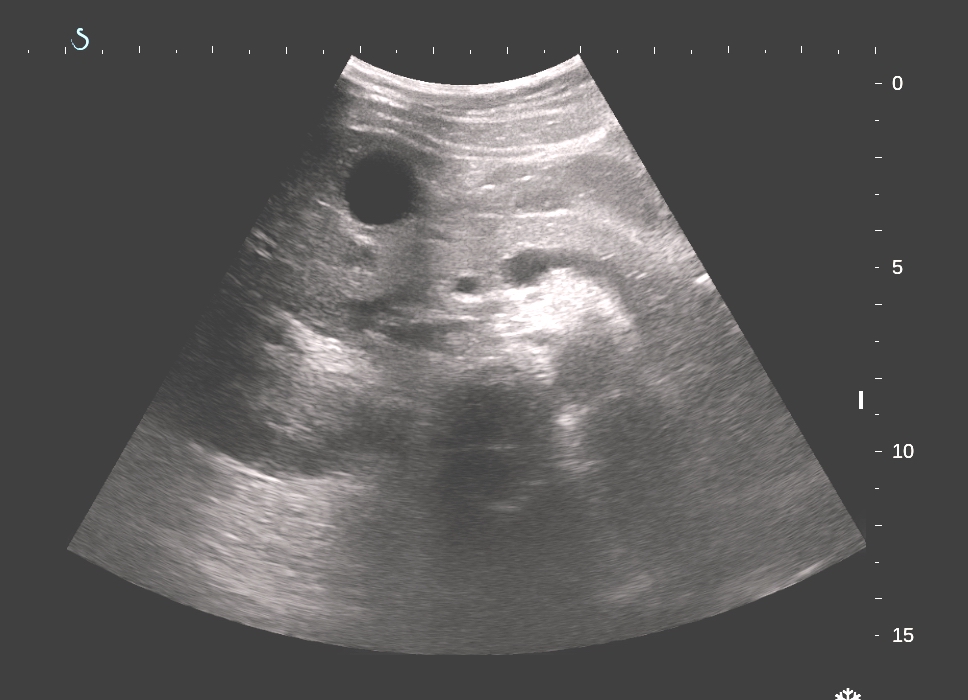
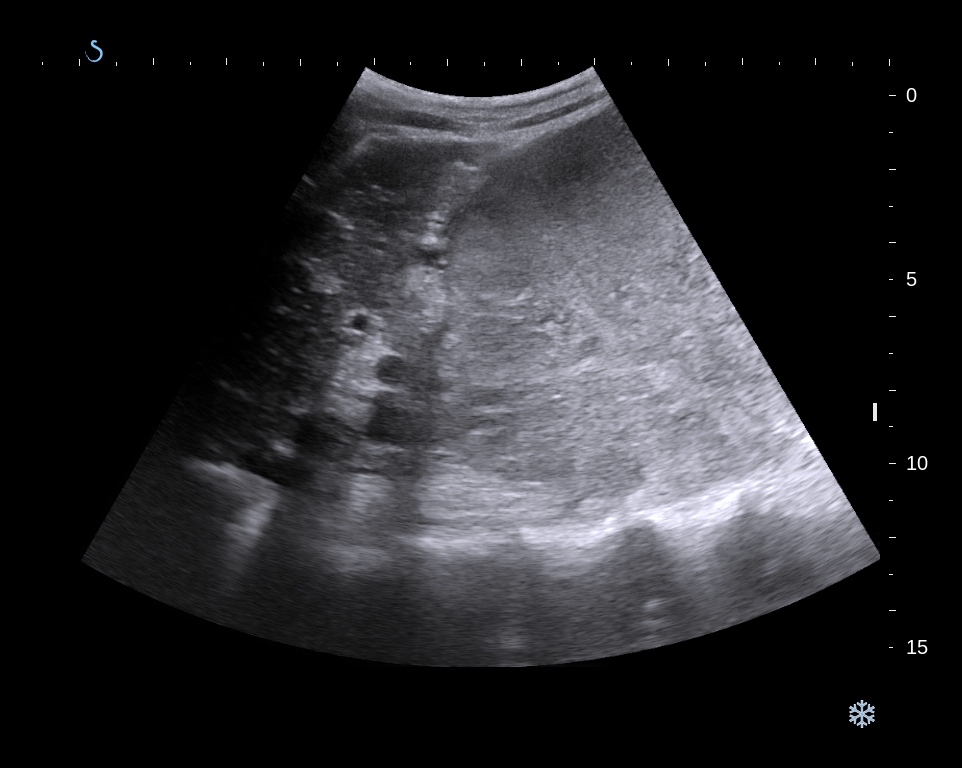
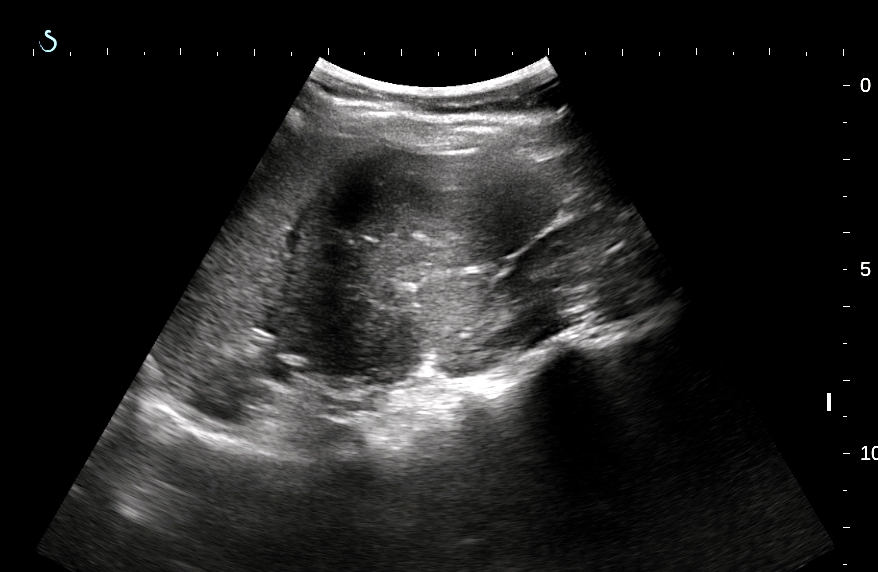
US 3 :sacrum and the mass.

Sonologist suggestion is cystic lymphangioma.
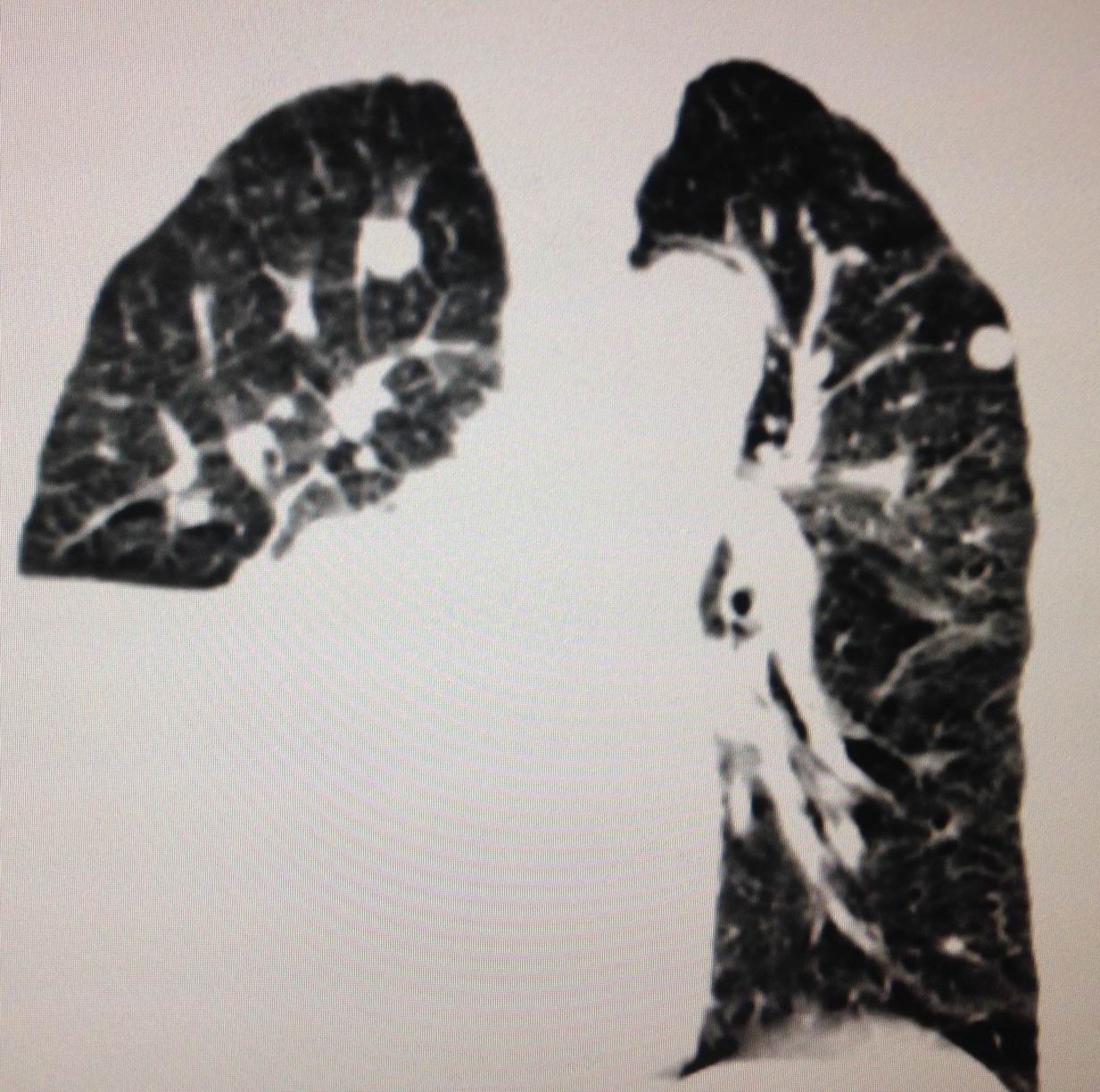
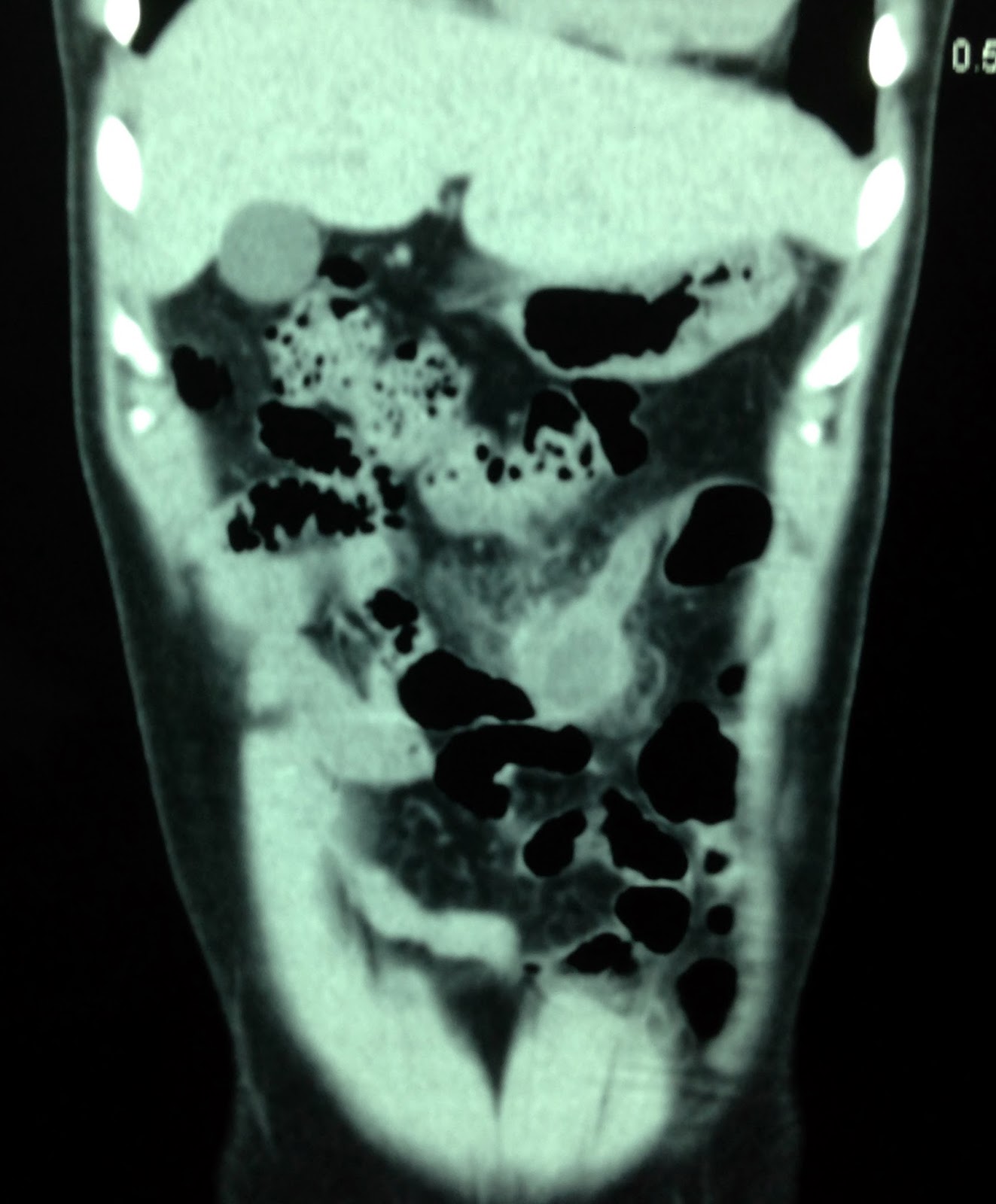
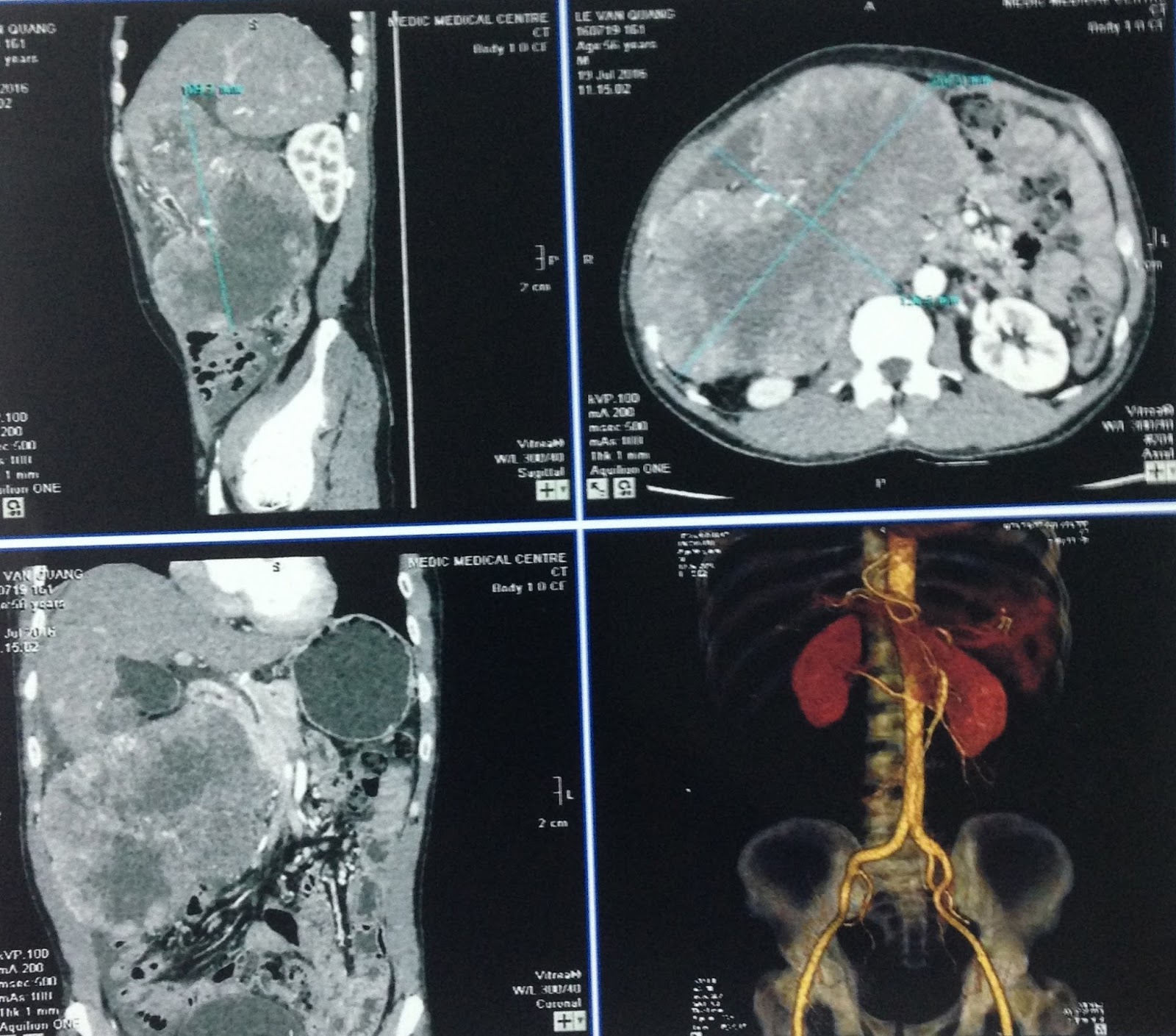
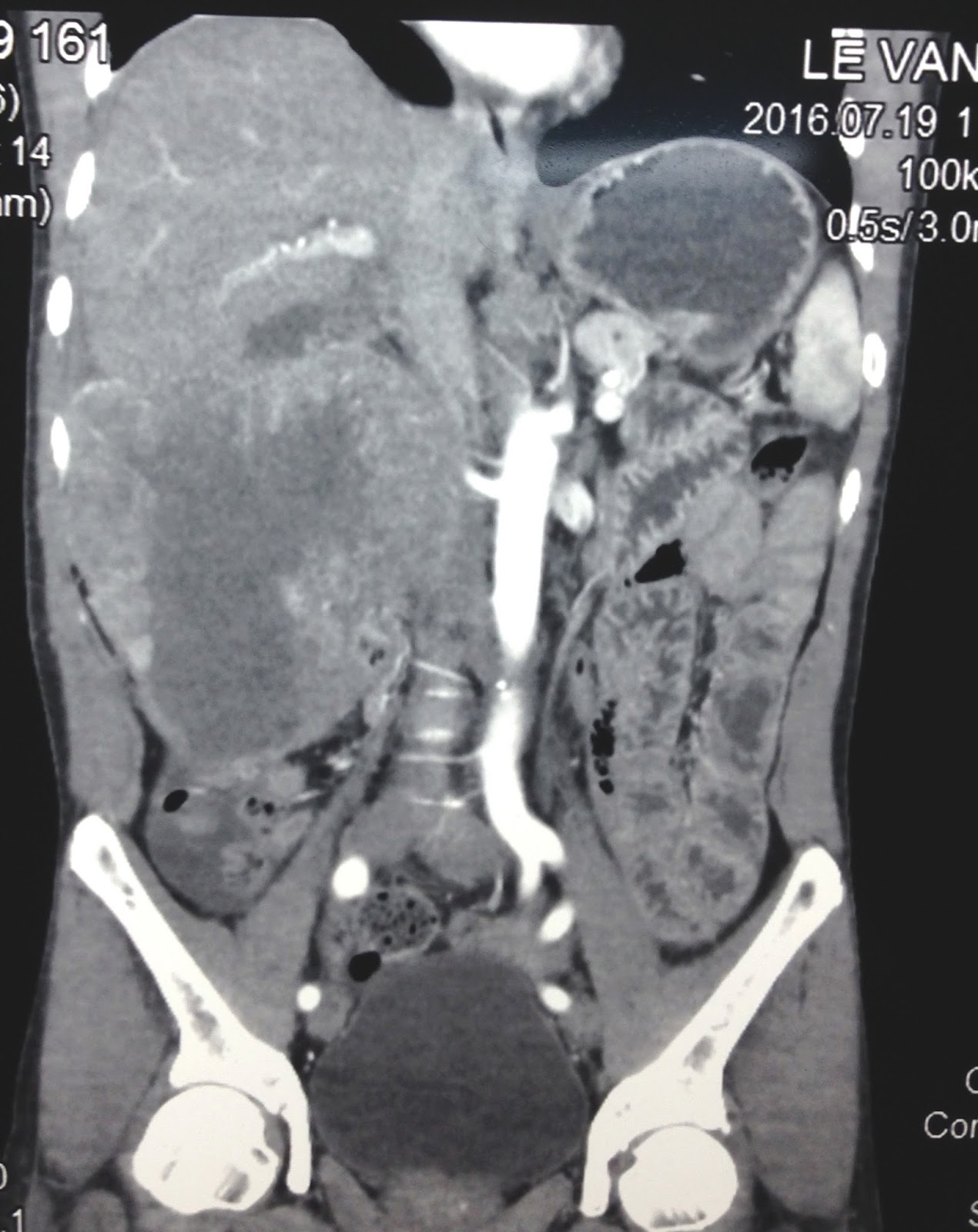
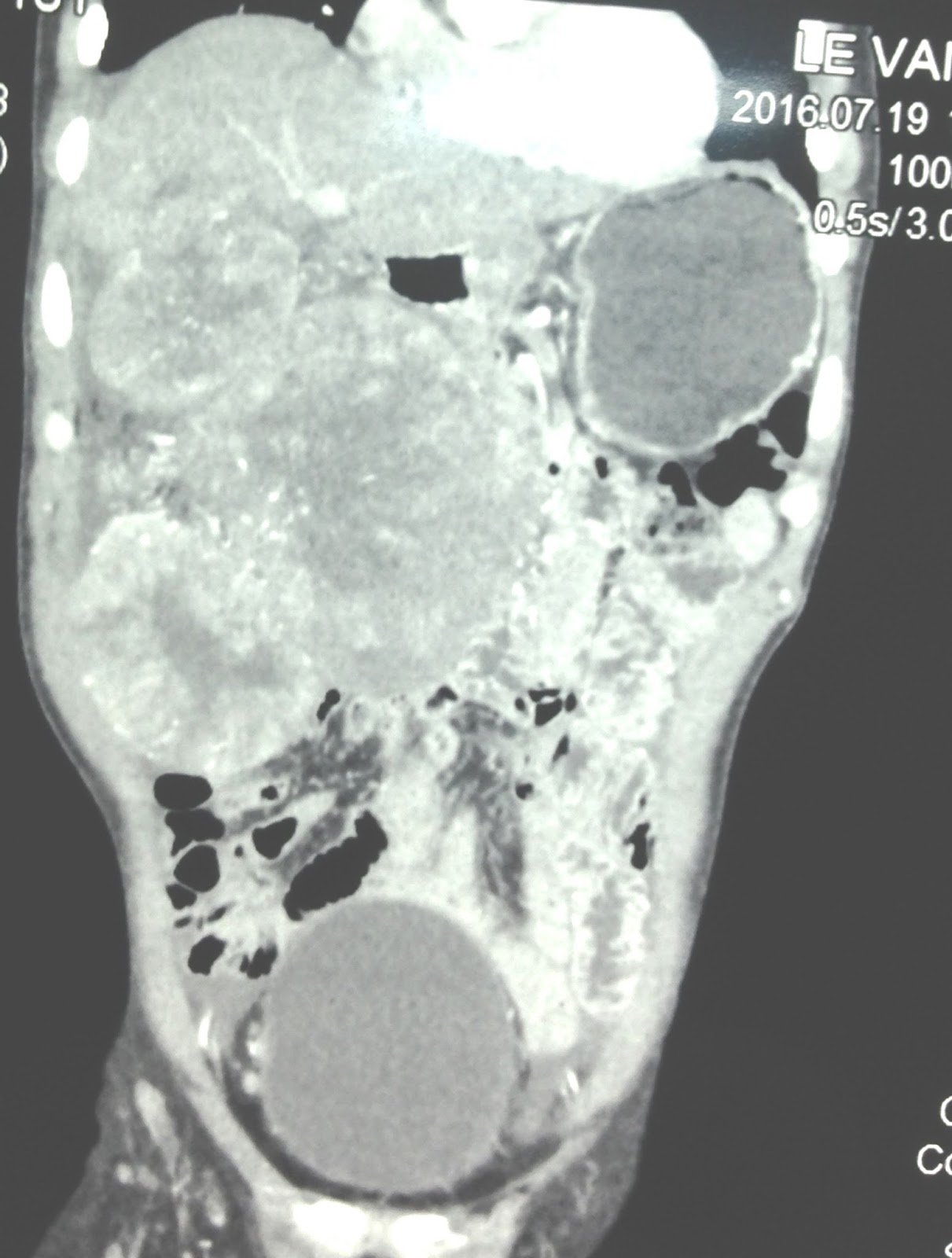
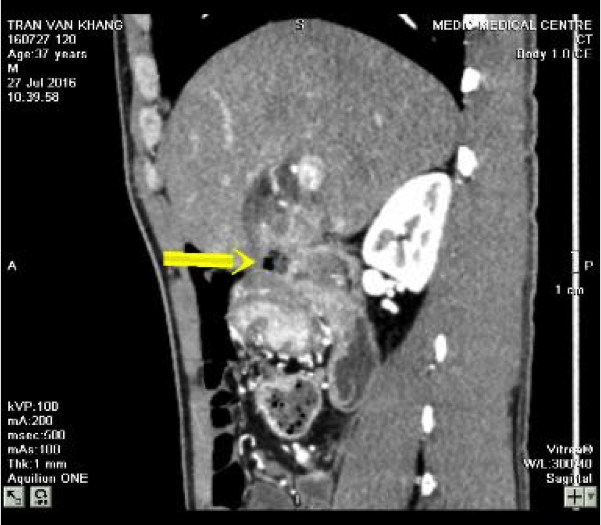
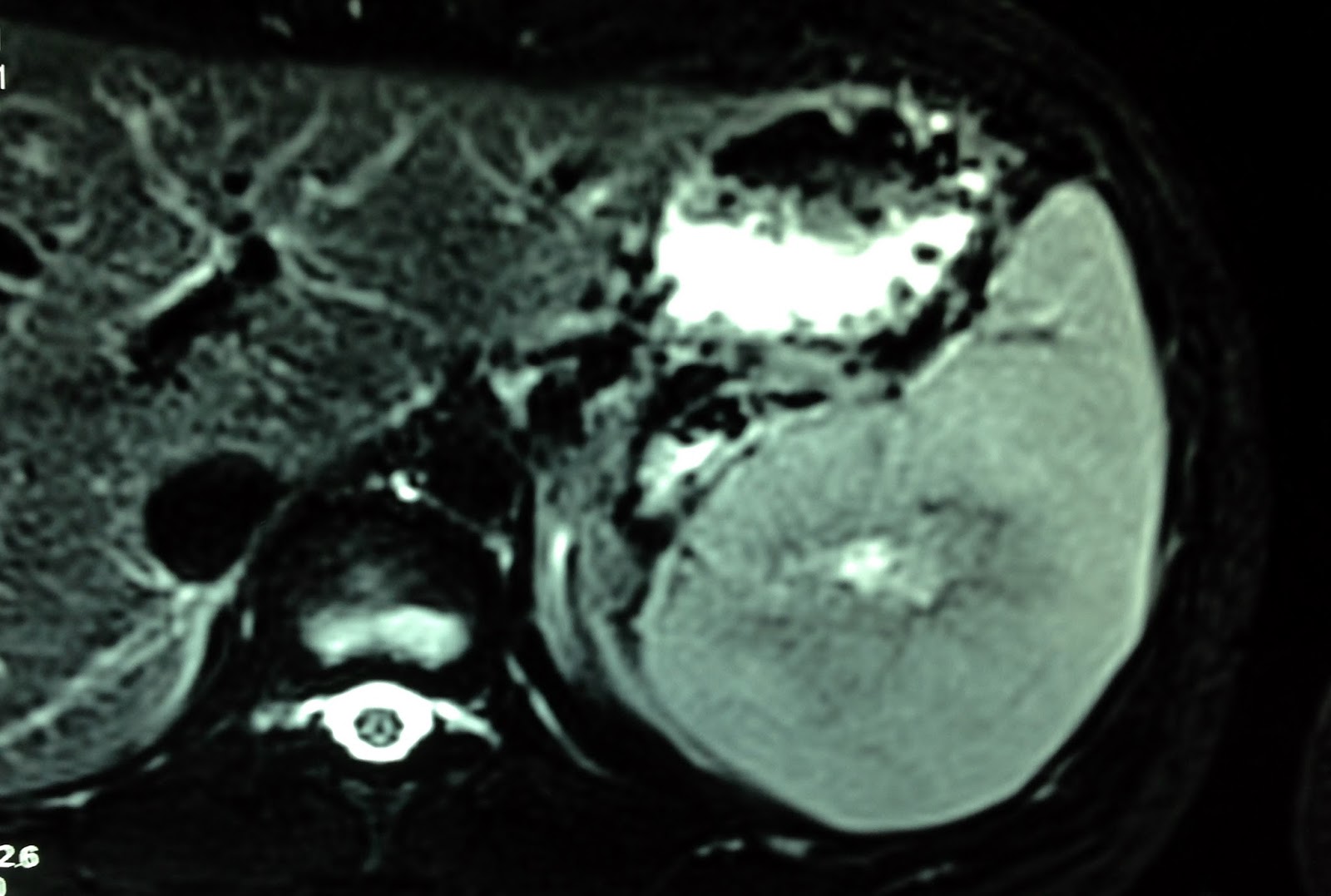
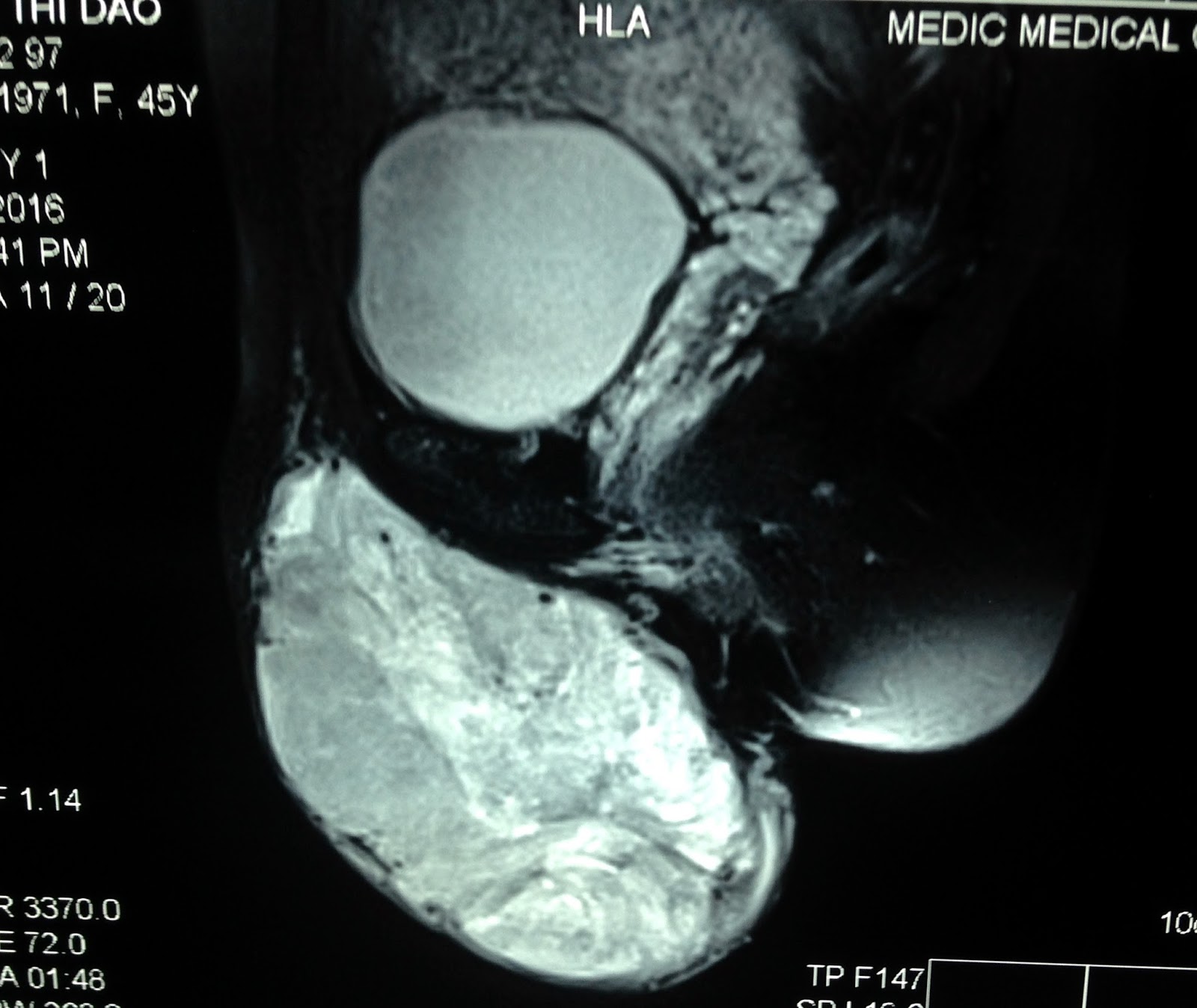
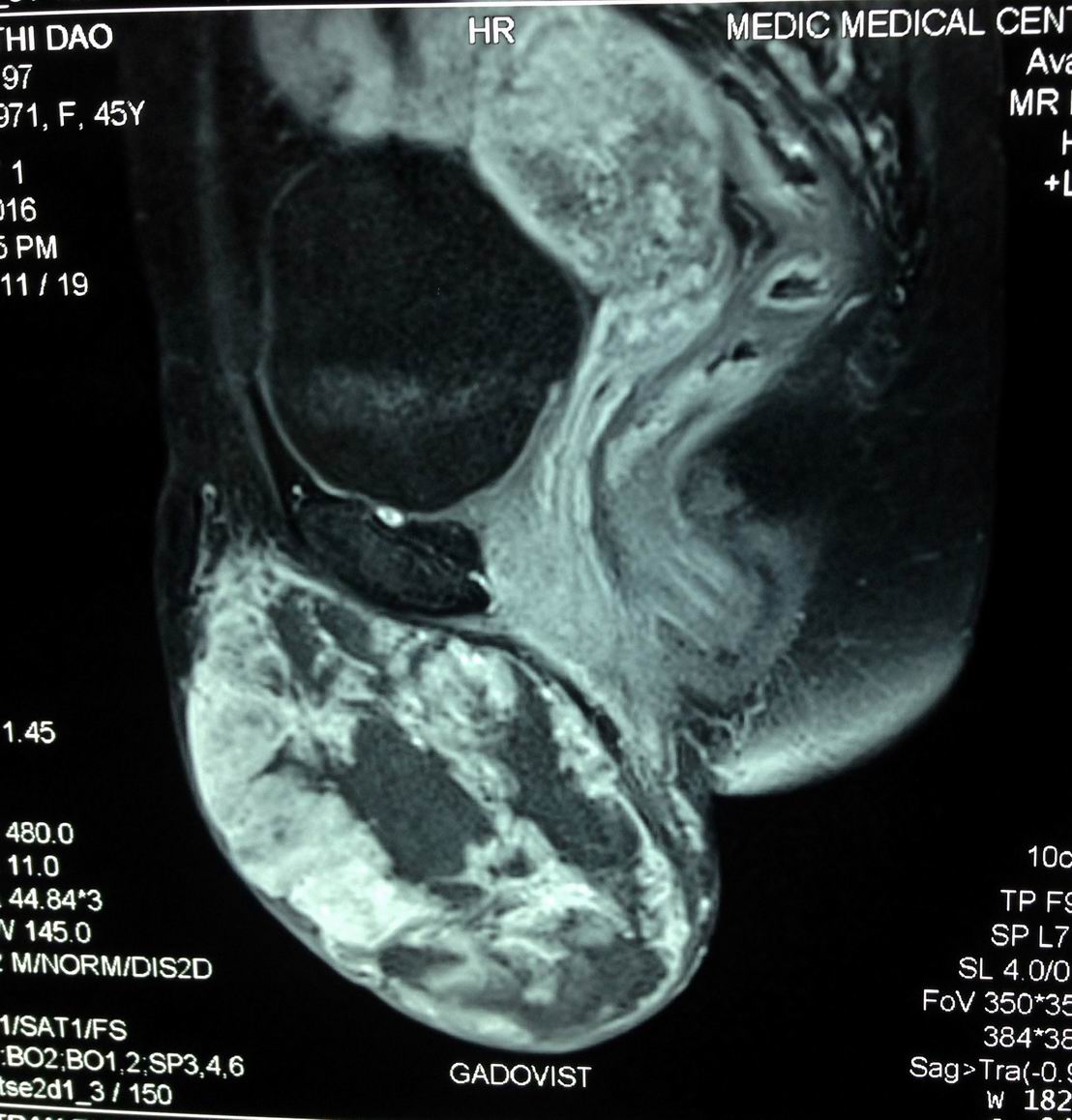
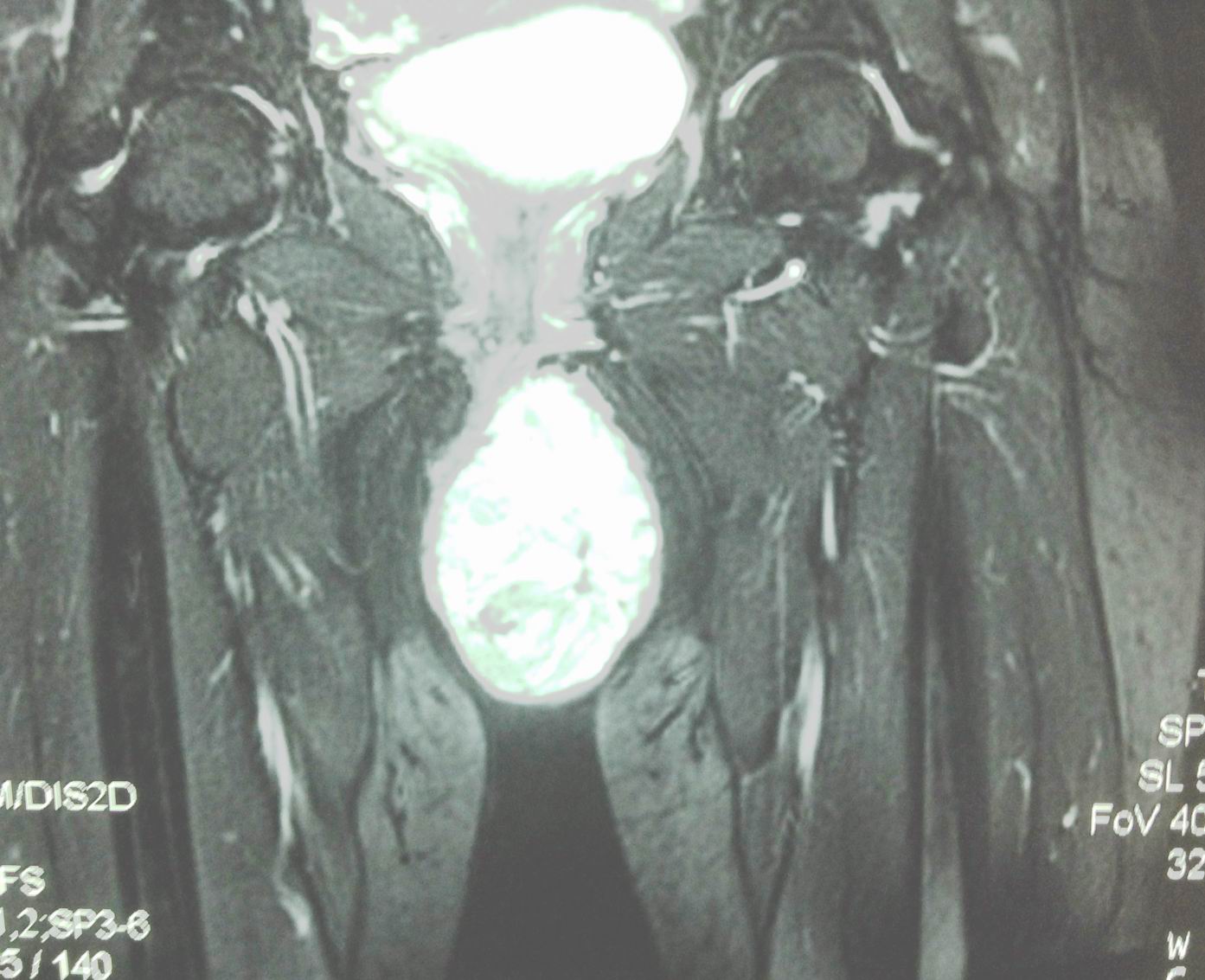
MRI report is fatty content, cystic part not connected to spinal canal.



Radiologist suggestion is sacro-coccygeal teratoma.
Operation removed this mass with solid structure and cystic part [see foto].
Report by surgeon is mature sacro coccygeal teratoma type 1.

MICROSCOPIC REPORT IS MATURE TERATOMA.